

The Hidden Cause of Your Chronic Coughing and Throat Clearing, and How to Fix It: Neurolaryngeal Hypersensitivity (NLH)
Do you have a continuous, irresistible urge to cough or clear your throat, even when you're not sick? Or, do you have odd sensations and even pain in your throat with no obvious cause? Maybe you've been told your lungs are clear, your reflux is under control, and your allergies aren't severe enough to explain your symptoms, yet the symptoms continue.
One possible explanation is a condition called “neurolaryngeal hypersensitivity” (NLH). NLH is an umbrella term that encompasses the following conditions:
Chronic cough (refractory or idiopathic)
Throat clearing
Muscle tension dysphonia (MTD)
Paradoxical vocal fold motion (PVFM)
Shortness of breath
Laryngospasm
Laryngeal pain (and other sensations: burning, tickling, pressure, etc.)
What Is Neurolaryngeal Hypersensitivity?
Let's break down the term:
Neuro = the nervous system and brain
Laryngeal = the larynx, also known as the voice box
Hypersensitivity = a heightened reaction to something that shouldn’t necessarily trigger a response
In people with neurolaryngeal hypersensitivity, the nerve that feeds into the throat and voice box (vagus nerve) becomes overly sensitive and creates danger signals in the brain that don’t actually need to be there. The body learns to interpret benign sensations in the throat that are even sometimes referred from the esophagus or ear, as a threat to the airway. That danger signal then triggers us to cough or throat clear, and/or creates uncomfortable sensations (even pain). Think of it like a smoke detector that has become too sensitive and starts going off when there's burnt toast instead of a real fire.
As a result, everyday activities and environmental exposures can trigger different sensations in the throat that lead to coughing and throat clearing.
NLH is and has been called many other things such as:
Neurogenic Laryngeal Hypersensitivity (Syndrome) NLH
Laryngeal Hypersensitivity
Sensory Neuropathic Cough
Chronic cough
Irritable Larynx Syndrome (ILS)
There is no agreed-upon terminology.
Scoping is Important:
Getting a baseline scope done by a voice-specialized ENT called a “laryngologist” is an essential first step in diagnosis to rule out other conditions that might be causing a cough or pain. You can read more about voice specialists and scope types here.
Conditions like vocal fold paralysis and paresis have a very high co-incidence of NLH because both of those conditions deal with the vagus nerve.
Getting scoped also allows us to actually see if mucus is on your vocal folds when you feel like it is. (It usually isn’t! The vagus nerve plays tricks on us in that way).
If you’ve been scoped and there is no obvious cause of cough and throat clear, you’re a great candidate for upper airway therapy. This should be done with a voice and airway-specialized speech-language pathologist.
Understanding Throat Function and Airway Danger:
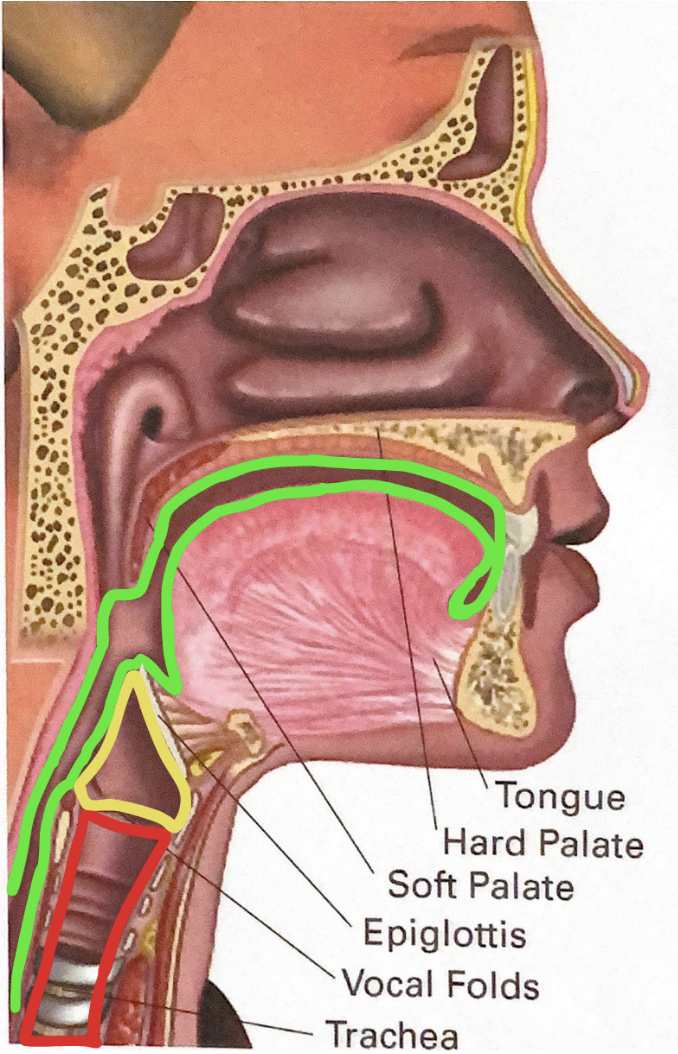
Understanding the TRUE danger zone of the throat can help your brain logically work around when and why certain sensations are safe. After your scope, it will likely have been determined that your airway is safe and there is no obvious mucus blocking the airway.
In the diagram below, any food, liquid, or mucus in the GREEN area is safe, and the natural response should be to swallow.
Any food, liquid, or mucus in the YELLOW area is still ok, and the natural response is to throat clear. However, swallowing should also clear content from this area.
Any food, liquid, or mucus in the RED area becomes a risk to the airway, and the natural response should be to cough.
A good rule of thumb is: if you can breathe, your airway isn’t obstructed. Teaching your brain that it’s safe can make it easier to replace coughing and throat clearing behavior.
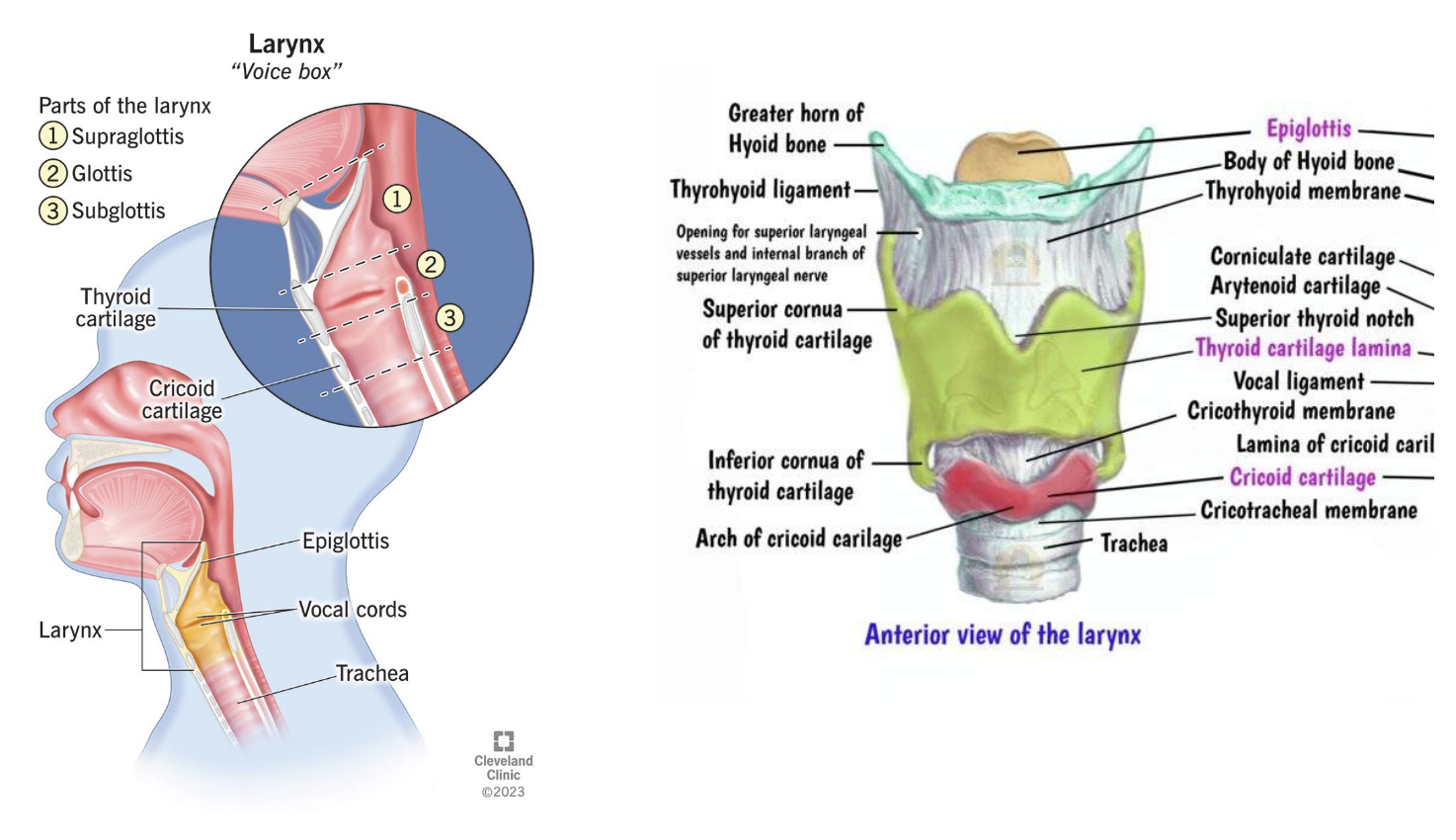
What is the larynx, and why is it important?
The larynx (also called the “voice box”) is a structure of five total cartilages that house our vocal folds (“vocal cords”). The vocal folds are the literal gateway to the airway. When we hold our breath, our vocal folds close, preventing air from coming in and out. When we swallow, our vocal folds and the “false folds” above them squeeze shut to make sure no food or liquid goes down our trachea and into the lungs. When our vocal folds are open, we are able to breathe. This helps us understand why our brain takes threats to the larynx seriously: if something is on the vocal folds, it can get into our airway, and keeping our airway clear and open keeps us alive.
What happens when you cough and clear your throat?
When something touches the vocal folds, it sends a signal to the sensory part of the vagus nerve (information that goes from our body to our brain) to tell the brain there’s something in the airway. Something touching the vocal folds triggers an automatic throat clear response, as an initial attempt to clear things out of the area. Once things pass below the vocal folds, the body should trigger an automatic cough response. The cough forces air up the trachea and through the vocal folds to dislodge or clear any blockage.
Coughing and throat clearing will occur for everyone at some point in their lives, because we all get sick or accidentally swallow things “down the wrong tube”. But, they should be occasional.
How it harms: The action of coughing or throat clearing slams the vocal folds together. Every time you do this, you create micro-tears in the mucosa (a slippery, thin tissue) on the top of the vocal folds. This slippery mucosa is important for allowing the vocal folds to vibrate together periodically, which in turn creates a clear voice. Therefore, if the mucosa is repeatedly getting damaged, you’re likely to have voice changes such as hoarseness and breathiness. This pattern of behavior can worsen lesions or create the development of lesions like polyps and nodules.
What is chronic cough?
Chronic cough is defined as a cough that has not resolved after 8 weeks. A refractory cough is a cough that has not responded to standard treatment, which usually consists of beta blockers and/or steroid inhalers. An idiopathic cough is a cough that has no known origin. A cough could only be deemed idiopathic if an exam of the larynx has been done with stroboscopy (a strobing light source), to make sure that there’s no other obvious problems. You can read more about the different types of laryngeal exams here.
There are many common causes of chronic cough such as asthma, acid reflux, and allergies, but the fact is that none of those conditions would be helped by coughing…
A nasty cycle:
When you feel a sensation in your throat or larynx, it sometimes triggers a cough or throat clear. If you let the coughing and throat clearing become habitual, you are creating repeated micro-tears in the mucosa. When you have micro-tears in the mucosa, your brain then interprets that irritation as something ON the vocal folds, when there’s not, which triggers another cough or throat clear.
So the cycle becomes:
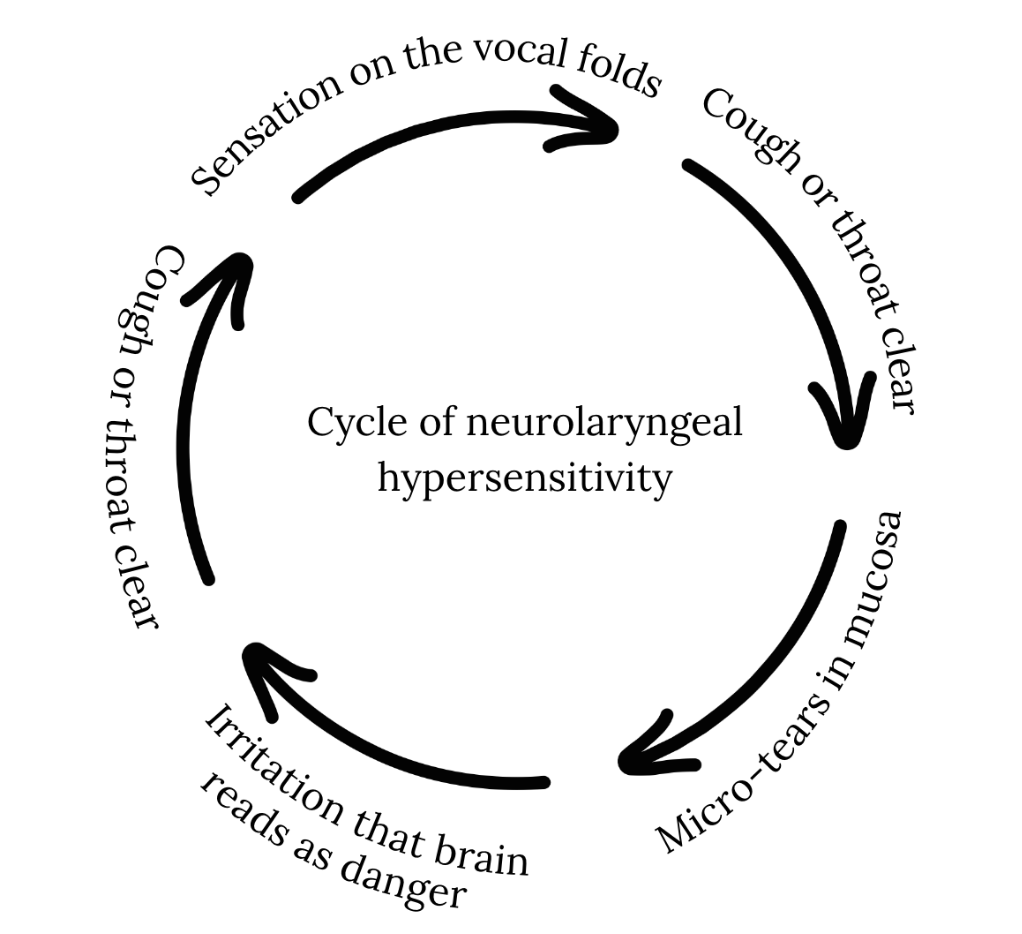
This cycle is neuroplastic, which means that the brain has now wired itself to respond to a pattern over time. The only way to get out of this cycle is to give your brain a new pattern to follow. Thankfully, because our brains are flexible, we can literally rewire our neurons to do something new!
Easier Said Than Done:
It might sound easier said than done to “rewire neurons”, and that’s because it is. The key to defeating NLH is to get comfortable sitting with uncomfortable sensations, and create enough of a pause to make a different choice.
Here’s how to do it!
Step 1: Identify Your Triggers
The nervous system learns patterns. One of the most important parts of treatment is learning what situations tend to trigger your symptoms.
Inhaled Triggers are things you breathe in that may irritate the sensitive nerves of the throat, which can include:
Dust
Smoke
Chemical odors
Bleach
Nail polish
Ammonia
Cleaning products
Laundry detergents
Soaps
Candles
Perfumes
Dry air
Cold air
Changes in humidity
Dry, particulate foods such as crackers or cookies
Mechanical Triggers are triggers that come from mechanical movement in the larynx, which is voicing! These can include:
Heavy breathing
Gasping
Laughing
Speaking loudly
Speaking for extended periods
Speaking in general
Singing
Singing higher pitches
Crying
Emotional Triggers are things that cause negative emotions such as:
Anxiety
Stress
Crowded environments
Emotional memories or associations
Talking about coughing
Step 2: Retrain Patterns by Learning Your "Red Zone":
Most people notice a “warning sign” just before they cough or clear their throat.
This is called the red zone- the moment when your nervous system is signaling that a cough is about to happen.
For example, you may notice:
A tickle in the throat
Tightness
An itch
A sensation of mucus
Pressure in the throat
One common warning sign is the feeling of mucus sitting on a "shelf" in the throat.
Your goal is to recognize this sensation as early as possible.
Journal Your Symptoms
For several days, try tracking:
What happened before the cough/what trigger was present?
What sensation did you feel immediately before coughing?
The more aware you become of your patterns, the easier it becomes to interrupt them.
Step 3: Replace the Behavior Instead of Reinforcing It
When you enter the red zone, the goal is to replace the cough or throat clear with another behavior.
Each time you successfully replace the cough, you teach your nervous system a new response pattern.
Helpful replacement strategies include:
Inhale gently through the nose, hold your breath, then swallow
Inhale through the nose and exhale through pursed lips
Take a sip of water
Perform a dry swallow
Chew gum
Suck on hard candy
Suck on ice
Use non-menthol cough drops (Luden’s, Halls Breezers, Fontus, Grether’s Pastilles)
Gentle humming
Breathing through a straw
Gentle gargling
Cup bubble exercises
Tongue-out swallow (“Masako” technique)
When you know you'll be around triggers, have your strategy ready before symptoms begin.
The “Hard Swallow” Technique
One particularly effective strategy is the hard swallow.
Follow these steps:
Inhale gently through your nose.
Hold your breath.
Take a small sip of water.
Swallow firmly, as though you're swallowing a peach.
This technique helps interrupt the urge-to-cough cycle and provides an alternative response for the nervous system.
Practice Before You Need It
Many people wait until they're actively coughing to try these strategies.
Instead, practice your preferred strategy five times per hour when you're not coughing or throat clearing.
Skills become more automatic when they're practiced in calm moments. The more familiar the strategy feels, the easier it will be to use when symptoms arise.
What If the Cough Happens Anyway?
Sometimes the cough breaks through despite your best efforts.
If that happens, try to regain control as quickly as possible:
Inhale gently through your nose.
Exhale slowly through pursed lips or on a gentle "shh" sound.
This can help shorten a coughing episode and prevent multiple coughs from occurring in a row.
Identify and Replace:
So, remember: IDENTIFY and REPLACE. Teach your brain to recognize the sensation you get in your throat before you cough or throat clear, and be ready to replace that sensation with a strategy you’ve already been practicing.
Retraining the Nervous System Takes Time:
Neurolaryngeal hypersensitivity is not simply a throat problem, it's a nervous system problem. Treatment focuses on increasing awareness of triggers, recognizing warning signs, and repeatedly practicing alternative responses.
Over time, many people find that their symptoms become less intense, less frequent, and easier to manage. Sometimes this happens immediately!
The key is consistency: identify, recognize, replace, and practice.
Laryngeal Pain and Other Sensations:
If you are not suffering from coughing and throat clearing, but are dealing with ongoing neurogenic laryngeal pain, burning, tickling, or other uncomfortable sensations, this is still neurolaryngeal hypersensitivity. Stay posted for a separate article specifically focused on addressing this subset of symptoms.
Sources:
Abdallah, S. J., & Smith, J. A. (2018). An update and systematic review on drug therapies for the treatment of refractory chronic cough. Expert Opinion on Pharmacotherapy, 19(7), 687–711.
Dąbrowska, M., Grabczak, E. M., Rojek, D., Łobacz, A., Klimowicz, K., Truba, O., Rybka, A., Krzeski, A., & Krenke, R. (2018). Speech therapy in the management of difficult-to-treat chronic cough: Preliminary results. Advances in Respiratory Medicine, 86(6), 268–274. https://doi.org/10.5603/ARM.a2018.0044
Goldberg, L. (n.d.). Neurogenic laryngeal hypersensitivity syndrome: A treatment protocol [Conference presentation].
Hull, J. H., & Menon, A. (2015). Laryngeal hypersensitivity in chronic cough. Pulmonary Pharmacology & Therapeutics, 35, 111–116. https://doi.org/10.1016/j.pupt.2015.08.008
Lee, B., & Woo, P. (2005). Chronic cough as a sign of laryngeal sensory neuropathy: Diagnosis and treatment. Annals of Otology, Rhinology & Laryngology, 114(4), 253–257. https://doi.org/10.1177/000348940511400401
Lilly, G. L., Carroll, T., Pietsch, K., Dhillon, V., Bryson, P. C., & Akst, L. M. (2025). Refractory chronic cough: A state-of-the-art review for otolaryngologists. Otolaryngology–Head and Neck Surgery, 172(2), 419–435. https://doi.org/10.1002/ohn.1019
Ryan, N. M., & Gibson, P. G. (2009). Characterization of laryngeal dysfunction in chronic persistent cough. The Laryngoscope, 119(4), 640–645. https://doi.org/10.1002/lary.20114

Brittani is a voice, swallow, and upper airway specialized speech-language pathologist (CCC-SLP) living and working in NYC. She specializes in working with singers with injury and works to encompass holistic practices for all clients including manual therapy, mindfulness and somatic awareness, and behaviorally-focused interventions.